The Question of Protein
I am everywhere surrounded by friends and family sprinkling protein powder onto their protein shakes and shoveling it into their mouths as they pump iron in an endless attempt to build muscle. The societal obsession with protein and muscle growth can be traced largely to Peter Attia, who in turn was influenced by Don Layman, a scientist with financial relationships with the National Cattlemen’s Beef Association and the National Dairy Council (AKA Big Meat) and who touts the more complete amino acid makeup of animal protein. Even my wife has joined the anabolic stampede, drawn in her case by the promise of early satiety and weight loss. Even I, in a prior post, had jumped on the protein bandwagon.
I want to take the question seriously, because it is genuinely two-sided, and the honest answer turns out to be more interesting and nuanced than either the protein evangelists or the protein abolitionists let on.
Growth that does not know when to stop
We start with the framework that Mikhail Blagosklonny called hyperfunction theory. Blagosklonny’s claim was that the growth programs that build you up during development do not switch off once you reach adulthood. They keep running. And many of the diseases of aging — atherosclerosis, hypertension, hyperinsulinemia, the proliferative cancers–are, on this view, what continued growth looks like in a body that no longer needs to grow. The same anabolic axis that builds tissue in a child and repairs muscle in an athlete is, when chronically engaged in midlife, the axis that may underwrite a measurable share of cancer and metabolic disease. (Blagosklonny himself took heroic doses of rapamycin for years and died of brain cancer; people said “thank goodness he was on rapamycin” rather than asking the obvious question of whether he caused his disease, but that is a digression.) The hyperfunction theory is relevant here because protein fuels growth. Could it be that our protein feeding frenzy is paradoxically a life-shortening intervention? The rest of this post is an attempt to answer that question.
The machinery: GH / IGF-1 / mTORC1
The lever under all of this is the growth-hormone / IGF-1 / insulin / mTORC1 axis–the primordial circuitry that decides whether a cell grows and divides or holds still and repairs itself. Valter Longo and Morgan Levine proposed that in midlife, sustained anabolic drive (high IGF-1, tonically activated mTORC1) promotes proliferation in cells that are already accumulating mutations.
Leucine, one of the branched-chain amino acids, is the most potent dietary activator of mTORC1 we know. In 2009 Christopher Newgard’s group ran targeted metabolomics on lean versus obese subjects and found that the signature most strongly tracking insulin resistance was not fat or carbohydrate but the BCAAs. Leucine, valine, isoleucine (6). Feeding rats a high-fat diet supplemented with BCAAs reproduced the insulin resistance of high-fat feeding alone, despite less food and less weight gain. Animal protein is rich in BCAAs; chronic excess in a body that is already insulin-resistant keeps mTORC1 switched on. So far, the hyperfunction theory holds.
The strongest evidence that the axis matters: knock it out
If growth signaling really drives the diseases of aging, then disabling it should be protective, and it is. GH-receptor-knockout mice share dysfunctional GH/IGF-1 signaling and live 30–60% longer than wild-type mice, with delayed tumors. The human counterpart is Laron syndrome (growth-hormone receptor deficiency), in which circulating IGF-1 is profoundly suppressed. In a cohort of 99 affected subjects in southern Ecuador followed by Longo for over two decades, there was one non-lethal cancer and zero cases of diabetes. Among matched relatives in the same villages eating the same food, cancer ran about 17% and diabetes about 5% (3). Strikingly, the Laron subjects are often more obese than their relatives. A population that is obese yet nearly cancer- and diabetes-free tells you that adiposity per se is not the connective tissue between metabolic state and cancer. The connective tissue is IGF signaling.
The dose-response is visible in ordinary people too. In the UK Biobank (n ≈ 412,645), each 5-nmol/L increment in circulating IGF-1 was associated with higher risk of breast, prostate, colorectal, melanoma, kidney, and thyroid cancers–though lung, ovarian, head-and-neck, and liver cancers ran the other way, a reminder that IGF-1 is not a uniform poison (4). In EPIC-Heidelberg, higher IGF-1 was associated with breast and prostate cancer, and–this is the crucial part — the relationship between IGF-1 and all-cause mortality was U-shaped: both the lowest and the highest quintiles carried excess hazard (5). Very low IGF-1 carries the costs of frailty and cardiovascular fragility; persistently high IGF-1 in midlife appears to drive the diseases of adulthood. The optimum sits in the middle and most likely drifts upward with age.
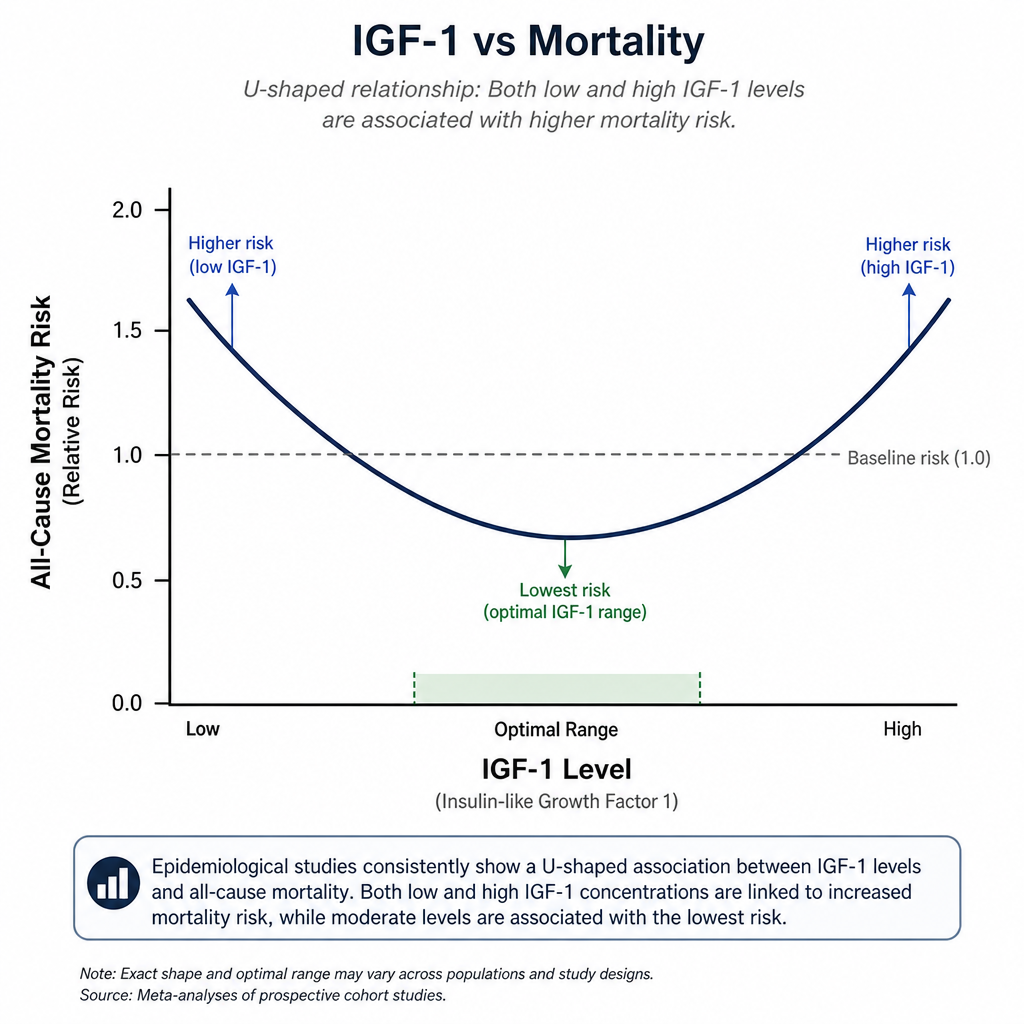
Hold on to that U-shape, because it does more work than it first appears. It means the goal is not to crush growth signaling as hard as possible. It means hitting a moving target and, as we will see, it is also the reason blanket protein restriction is the wrong tool.
Does it show up at the dinner table?
Levine and Longo went on to do an analysis of NHANES III, retrospective data covering 6,381 American adults aged 50 and over (1). Among 50–65 year-olds, high animal protein intake was associated with a 75% increase in all-cause mortality and a roughly four-fold increase in cancer mortality over 18 years; plant protein carried no such signal. But after age 65 the direction flipped: high protein was associated with lower all-cause and cancer mortality. Longo suggested that with age, IGF-1 falls as growth-hormone secretion declines (somatopause) and anabolic resistance sets in, so that sarcopenia and frailty, rather than proliferation, become the life-limiting risks. The same signal that is dangerous early becomes protective late. By that logic, eating a lot of protein in midlife is bad, but in old age it is protective. I should mention that NHANES is a single cohort built on one 24-hour dietary recall, with modest numbers and wide confidence intervals in the relevant strata, and it has never been cleanly replicated. It is the best single piece of evidence for an age-dependent flip, and it deserves real skepticism.
The Harvard Nurses’ Health Study and Health Professionals Follow-up Study are stronger — 131,342 participants, up to 32 years of follow-up, repeated diet assessments (2). Each 10% of calories from animal protein was associated with about 2% higher all-cause and 8% higher cardiovascular mortality; each 3% from plant protein with about 10% lower mortality; and substituting plant for animal protein (especially processed red meat) with substantially lower mortality. Critically, the animal-protein signal was concentrated in people who already had another risk factor–smoking, heavy drinking, obesity, inactivity. In otherwise healthy people it was weak. That is a clue we will need shortly.
The complication: total protein is not the villain
If you stop at Levine and Harvard, you conclude that protein shortens life. But that conclusion is complicated by the wider literature. A 2020 systematic review and dose-response meta-analysis in the BMJ pooled 31 prospective cohorts and roughly 715,000 participants with up to 32 years of follow-up (8). Highertotal protein intake was associated with lower all-cause mortality, not higher. Plant protein was associated with lower all-cause and cardiovascular mortality. And animal protein, taken on its own across these cohorts, was not significantly associated with cardiovascular or cancer mortality.
So in view of the current evidence, the signal seems to show that plant protein is better than animal protein. And recall the Harvard clue: the animal-protein harm clustered in people with other risk factors. Read together, these say that much of what looks like a protein effect is really the effect of the foods animal protein arrives in and the company those foods keep (processed meat, low fiber, the rest of an unhealthy pattern) rather than the protein molecule itself. It’s hard to make any conclusions at this point about a late life shift as Longo had hypothesized, since his findings have not been replicated.
It is also worth correcting any assumption that less protein is safer. Studies using the indicator amino acid oxidation method estimate average protein requirements above the current RDA of 0.8 g/kg/day in both younger and older adults (9). Low muscle mass and low strength are themselves robust predictors of mortality across all of adulthood, not just after 65, which is why geriatric consensus bodies such as PROT-AGE and ESPEN recommend 1.0–1.2 g/kg/day or more for older people, and more still for those who are active or ill. The danger at the end of life is not protein excess; it is protein deficit.
Why plant protein behaves differently
Plant protein is relatively low in BCAAs, and while both plant and animal protein raise IGF-1, plant protein does so less. More interestingly, animal protein is associated with lower IGF-binding protein (which frees more IGF-1), whereas plant protein is associated with higher IGFBP (which sequesters it). A cross-sectional study of 292 British women found vegans had about 13% lower serum IGF-1 and 20–40% higher IGFBP than meat-eaters (7). Again, low IGF-1 is not automatically better (refer to the curve above), but since most of our obese society is on the upslope of the curve, a plant based diet makes more sense.
Putting it together
Four lines of evidence converge on a narrower claim than “eat less protein.” Mechanistically, IGF-1/mTORC1 is a real driver of proliferation and the human genetics (Laron, GHR-knockout mice) prove the axis matters with near-perfect penetrance. The biomarker data (UK Biobank, EPIC) show IGF-1 tracking with epithelial cancers along a U-shaped mortality curve. The metabolomics (Newgard) implicate BCAAs, which animal protein supplies in abundance. And the epidemiology shows that the source of protein, not its mere presence, carries the risk. Total protein, if anything, appears to be protective.
Reconciling all of this gives a single coherent story. The thing you want to avoid is chronically high anabolic drive in midlife from BCAA-rich animal sources. Particularly processed and red meat, and especially if you already carry metabolic risk and are clearing those amino acids poorly. The thing you do not want is to slide down the left arm of the U-curve into frailty by under-eating protein, especially as you age. Dietary protein turns out to be a fairly weak lever on circulating IGF-1 in the first place, which is exactly why crude protein restriction is the wrong instrument: it barely moves the variable you care about while reliably costing you muscle.
What this implies in practice based on our current understanding
- In midlife, try to stick to plant based protein and avoid red meat. (There are other reasons to avoid beef, such as the bovine leukemia virus as well as the impact of the cattle industry on climate) Substitute plant protein for processed and red meat where you can. This is the move with the most consistent mortality evidence behind it.
- Keep total protein adequate to generous: roughly 1.0–1.6 g/kg/day depending on activity. The goal is choosing better protein, not eating less of it. Protein’s satiety and weight-loss benefits are real, and adequate protein protects lean mass during weight loss.
- Train against resistance. Exercise lets you spend the anabolic signal building useful tissue rather than leaving mTORC1 idling, and it lets you do more with less protein.
- At all costs avoid anabolic and androgenic steroids.
- Reserve real concern for the genuine excess case: large amounts of BCAA-rich animal and supplemental protein in someone who is already insulin-resistant or carrying other risk factors. Whey and BCAA supplementation past the point of building the muscle you need (and androgenic/anabolic steroids at any point) are plausibly life-shortening.
- After roughly 65–70, or in anyone showing early sarcopenia, the calculation inverts. Frailty kills, IGF-1 has already fallen, and protein adequacy becomes protective. This is the time to err generous.
So should you limit all protein before old age, or only animal protein?
Only animal protein, and even that is really a statement about food sources and the company they keep, not about protein as a molecule. Limiting all protein in midlife is the one strategy the data do not support: it does little to lower the IGF-1-related risk that comes specifically from animal sources, while it undermines the muscle mass and strength that independently predict survival and become so much harder to rebuild later. The U-shaped curve makes the point on its own. If both tails are dangerous, the answer was never “as little as possible.” “Limit animal protein, especially the processed kind, in midlife, and keep total protein adequate” is consistent with the evidence.
References
- Levine ME, Suarez JA, Brandhorst S, et al. Low protein intake is associated with a major reduction in IGF-1, cancer, and overall mortality in the 65 and younger but not older population. Cell Metab. 2014;19(3):407-417. doi:10.1016/j.cmet.2014.02.006
- Song M, Fung TT, Hu FB, et al. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern Med. 2016;176(10):1453-1463.
- Guevara-Aguirre J, Balasubramanian P, Guevara-Aguirre M, et al. Growth hormone receptor deficiency is associated with a major reduction in pro-aging signaling, cancer, and diabetes in humans. Sci Transl Med. 2011;3(70):70ra13. doi:10.1126/scitranslmed.3001845
- Knuppel A, Fensom GK, Watts EL, et al. Circulating insulin-like growth factor-I and risk of 19 site-specific cancers: UK Biobank analyses. Cancer Epidemiol Biomarkers Prev. 2020;29(8):1531-1540.
- Kaaks R, Johnson T, Tikk K, et al. IGF-1 and risk of morbidity and mortality from cancer, cardiovascular diseases, and all causes in EPIC-Heidelberg. J Clin Endocrinol Metab. 2023;108(10):e1092-e1105.
- Newgard CB, An J, Bain JR, et al. A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009;9(4):311-326.
- Allen NE, Appleby PN, Davey GK, et al. The associations of diet with serum insulin-like growth factor I and its main binding proteins in 292 women meat-eaters, vegetarians, and vegans. Cancer Epidemiol Biomarkers Prev. 2002;11(11):1441-1448.
- Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ. 2020;370:m2412. doi:10.1136/bmj.m2412
- Bauer J, Biolo G, Cederholm T, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013;14(8):542-559 (see also indicator amino acid oxidation requirement studies, e.g. Rafii M, et al. J Nutr. 2015).